
Advertisement

A novel approach to combat the spread of coronavirus and other respiratory infections with the aid of a smart sanitizing respirator

HTML
2056
Total
527
Citations
Copyrights: Raj K Gandhi, 2023. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
In spite of social distancing, isolation at home, quarantine, use of face masks, and total shutdowns of cities, states, and countries COVID-19 has spread to infect nearly 150 million people and killed more than 3 million including many thousands of health care workers around the world in the course of 1 year. This invisible enemy like many other respiratory viruses spreads from person to person largely through airborne droplets or microdroplets.
If we had a respiratory device to wear that would disinfect and sanitize each breath before we breathe in and also disinfect and sanitize each breath we breathe out before it is discharged back into the air, we will be able to stop the airborne spread of respiratory infections. Such a device will obviate the need for total isolation at home and mass quarantines in ships or military bases. If you are sick with an acute respiratory infection, you will stay at home if the illness is mild or moderate and in the hospital if it is severe. If you have been exposed to coronavirus or suspected of having been exposed but have no symptoms, you should be able to go about your normal business while wearing this device. Same should apply if the symptoms are mild and/ or infection is with “flu” or common cold virus. The schools will stay open and there will be no need to close a town, city, a region, or an entire country. The anxiety and fear will be minimized. Health care workers will greatly benefit from this device and will not have to wear suffocating masks like N-95 respirator. During activities that pose high risk of aerosol transmission such as coughing, endotracheal intubation, bronchoscopy, suctioning, cardiopulmonary resuscitation, or disconnecting the ventilator, this device will provide near-total protection to the health care workers.
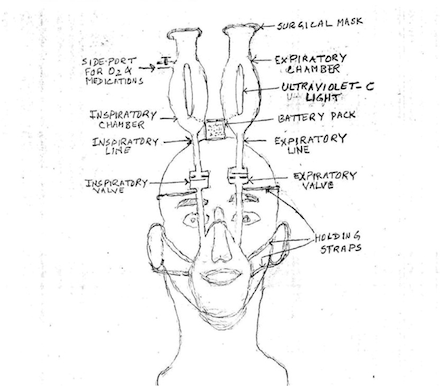
In the following paragraphs, I will describe the design of this device along with a conceptual sketch. I will also try to explain the structure and function of each component.
1. Face mask: It will be light and soft and pliable, preferably made out of transparent silastic. It will fit snugly over the mouth and nose allowing nearly zero air leak around it.
2. Connecting tubes: There will be two tubes coming out of the upper front part of the mask, and they will be labeled “Inspiratory line” and “Expiratory line.” They will go straight up over the forehead and curve around the frontal part of the skull going backward on the top of the skull. The inspiratory line will be connected to a one-way valve which will allow the air to flow in for inspiration. This valve will shut down during expiration. The expiratory line will be connected to a one-way valve which will allow the air to flow out during expiration. This valve will shut down during inspiration. Beyond the valve, each tube will be connected to a very light weight oblong flask which will be called “Sanitizing Chamber.” Each sanitizing chamber will be further identified as inspiratory or expiratory based on its connection.
3. Each sanitizing chamber will be about 6–10 inches tall with the shape of a flask and has an internal volume of about 1500 ml. In the center of each chamber, there will be a low-voltage light fixture holding a long thin bulb that will emit ultraviolet-c light (wavelength 250– 280 nm) when turned on. A battery cell will supply the power for this light. This light will continually sterilize the air around it inside the sanitizing chamber. The walls of the sanitizing chambers will be either made of aluminum or have a thin internal coating of aluminum to reflect the ultraviolet light all inside, to maximize its sterilizing effect.
4. The top of the sanitizing chamber will be the open end like the mouth of a flask. It will be a wide mouth and will be covered with a surgical mask, preferably made out of triple layer of cotton gauze. This mask will be changed every 8 h when in use. For extra safety during an epidemic or high flu season, double mask cover can be used.
5. The inspiratory chamber will have a side port with an on and off stopper on it. This port will be used for delivery of oxygen and/or medications if needed.
An average healthy adult male breathes in and breathes out about 500 ml of air with each breath and at rest, his respiratory rate is about 12–15 breaths/min. At the rate of 15 breaths/min, he takes in 500 ml of air every 4 s or so and exhales the same volume every 4 s. The sanitizing chamber of this respirator will hold about 1500 ml of air from which 500 ml will be inhaled every 4 s and replaced by the same amount of atmospheric air filtered through the surgical mask. If the sanitizing chamber was smaller and could hold only 500 ml, the air being inhaled would be exposed to ultraviolet light only for 4 s before being inhaled. This will be too short to achieve satisfactory sanitization. Ultraviolet light takes 10–15 s to sterilize the air in its vicinity.[1-5] With 1500 ml of air in the sanitizing chamber, each breath of 500 ml would have been exposed to ultraviolet light for at least 12 s before being inhaled. An average healthy adult female breathes in and breathes out about 400 ml of air with each breath at rest, and her respiratory rate is about 14–15/min. With mild exercise like slow walk during grocery shopping, it may go up to 18–20/min. So for women, a sanitizing chamber of 1500 ml will be sufficient and adequate. For men, sanitizing chambers of 2000 ml capacity will be better. It will be no problem to make these devices in two sizes. In fact, a third size with 2500 ml capacity sanitizing chambers for extra-large persons will not pose much of a problem to make. Similarly, two or three smaller sizes will be made for children.
There are some more advantages to using this device. The air going into the lungs of the user will be first filtered by the surgical mask and then sterilized by the ultraviolet light.[1-5] It will also enter the sanitizing chamber at a higher level where the air would be relatively clean and free of droplets hanging up in the air. Hence, if the user is healthy and is worried about catching an airborne infection like coronavirus, say in a mall or grocery store, he/she needs not worry at all because the air he/she will be inhaling, will have been sterilized in the inspiratory chamber with the help of ultraviolet-c light. [1-5] Moreover, if he/she were infected, he/she would not pose any risk to others because the air he/she would be exhaling would have been sterilized in the expiratory chamber before getting out. Since most people are healthy and will be using these respirators prophylactically, they will be sanitizing the air continually with each breath, thus helping the environment.
This respirator can provide some more therapeutic benefits. Through the side port of the inspiratory chamber, supplemental oxygen can be given easily without wasting any oxygen into the atmosphere as it happens with nasal cannula or a face mask. Someone with a respiratory rate of 20/min and tidal volume of 500 ml will be breathing in and out 10 L of air every minute. Oxygen through the side port of the inspiratory chamber at the rate of 1 L/min will supply 10% supplemental oxygen. At 2 L/min, it will go up to 20% and so on. In early stages of respiratory infection with coronavirus perhaps, this is all one would need in addition to other supportive measures. It will be possible to provide this kind of care at home to most patients, thus avoiding the need for hospitalization. Home health care workers, respiratory therapists, and nurses will be able to monitor the progress of such patients mostly through telephone and sometimes by home visits if needed. Patients and their families can be trained easily to check their vital signs and even oxygen saturation on daily basis and report to their health-care provider. Only very seriously sick patients requiring mechanical ventilation and/or other intensive therapeutic measures will need hospitalization.
Some more benefits will be realized from this respirator after it has been in use for some time. For example, it may be possible to deliver oxygen and/or other therapeutic agents into the bronchopulmonary segments with greater efficiency than the modalities in use at present. In the future, when some safe antiviral/antibacterial agents become available for pulmonary use, it will be possible to deliver them directly into the respiratory passages and lungs through the inspiratory chamber. With the help of this device, the treatment of other respiratory ailments such as bronchial asthma and emphysema might also become more efficient.
It will be easy to clean this respirator and all its components at the end of the day or as and when needed. The only disposable component is the surgical mask covering the mouth of each sanitizing chamber. Even that can be washed and reused, if it is made of triple layer of cotton gauze as recommended by me. The respirators used in the hospital to treat sick patients will of course be discarded and disposed of.
Will it be possible for this device to show some curative potential for patients with COVID-19 or flu or other respiratory infections? That will be a bonus to hope for. Only time will tell. It will, however, be quite possible and very likely that the number of flu cases each year will be reduced significantly with the help of this device, thus reducing the number of flu deaths also. That in itself will be a great achievement considering the yearly incidence and fatality rate of flu.
This respirator will make it possible for an “ambulatory isolation” in place of quarantine at home or some other place. Most workers will, therefore, be able to go back to work wearing this respirator. There will be no need to close manufacturing or meat processing plants. It seems that this respirator has the potential of altering the course of an epidemic with a respiratory virus and not only save lives but also the economy and the livelihood of millions of people.
This article was published by Scientific Scholar and has been archived here.
References
- Welch D, Buonanno M, Grilj V, Shuryak I, Crickmore C, Bigelow AW, et al. Far-UVC light: A new tool to control the spread of airborne-mediated microbial diseases. Sci Rep. 2018;8:2752.
- Frequently Asked Questions/American Ultraviolet. Available from: https://www.americanultraviolet.com/faq-germicid
- Nakamura H. Sterilization efficacy of ultraviolet irradiation on microbial aerosols under dynamic airflow by experimental air conditioning systems. Bull Tokyo Med Dent Univ. 1987;34:25-40.
- University of California-Santa Barbara. Ultraviolet LEDs Prove Effective in Eliminating Coronavirus from Surfaces and Potentially, Air and Water. 2020. United States: Science Daily; Available from: https://www.sciencedaily.com/releases/2020/04/200414173251.htm [Last accessed on 2020 Apr 14]
- Britannica. 2020. Encyclopedia Britannica. Available from: https://www.britannica.com/biography/Niels-Ryberg-Finsen [Last accessed on 2021 Aug 03]
Comments & Peer Review
Must Read
Downloads
Article Details
How to Cite
Publication history
Published: 07-02-2022
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
JMRI Journal
Search for this article in:
Google Scholar
Researchgate
CNKI Scholar